
Sally shows why it helps to notice your breast-belly contour (as well as the direction your nipples look) as you prepare to breastfeed
It helps to notice your breast-belly contour
Our breast-belly contour is the contour or shape outline we have when looking at our body in a semi-reclined position from the side. Imagine drawing a line to show what you'd see if you were looking at your body side-on, from over and then under your breast, and down the upper part of your tummy.
Sallly's breast-belly contour
In the following sketch, Sally is lying back at about 45 degrees, semi-reclined so that she can breastfeed her baby.
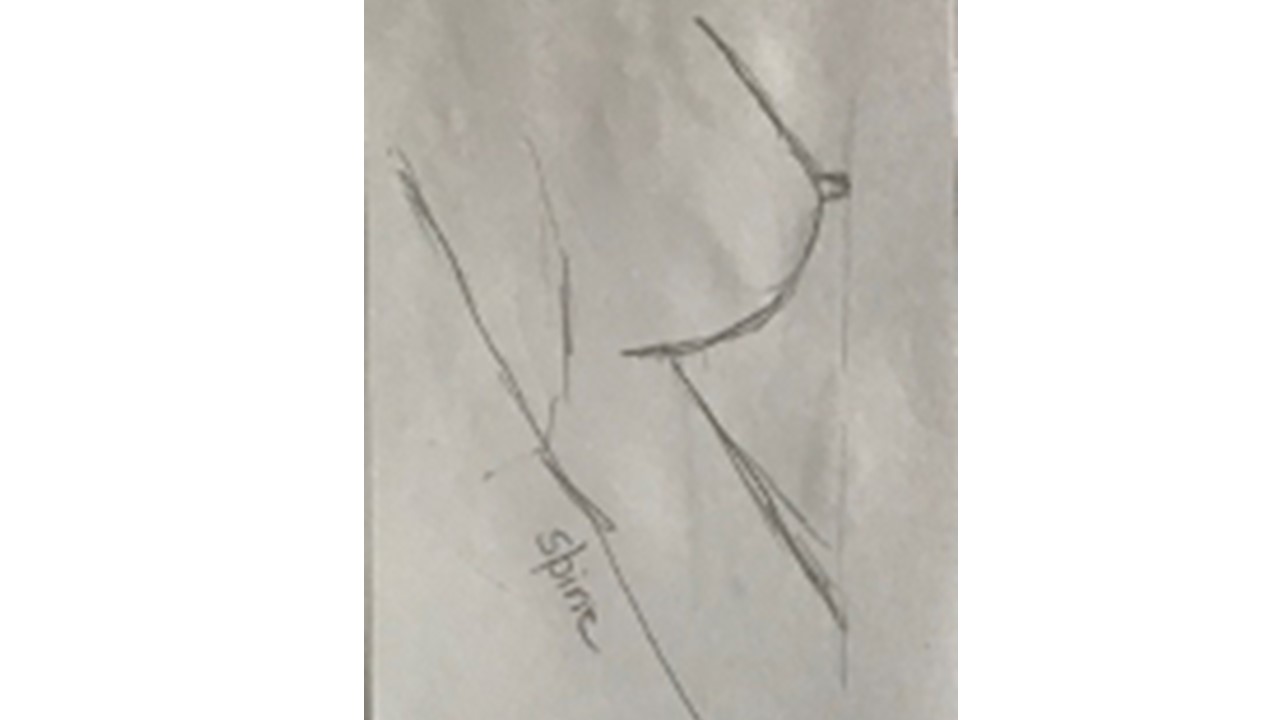
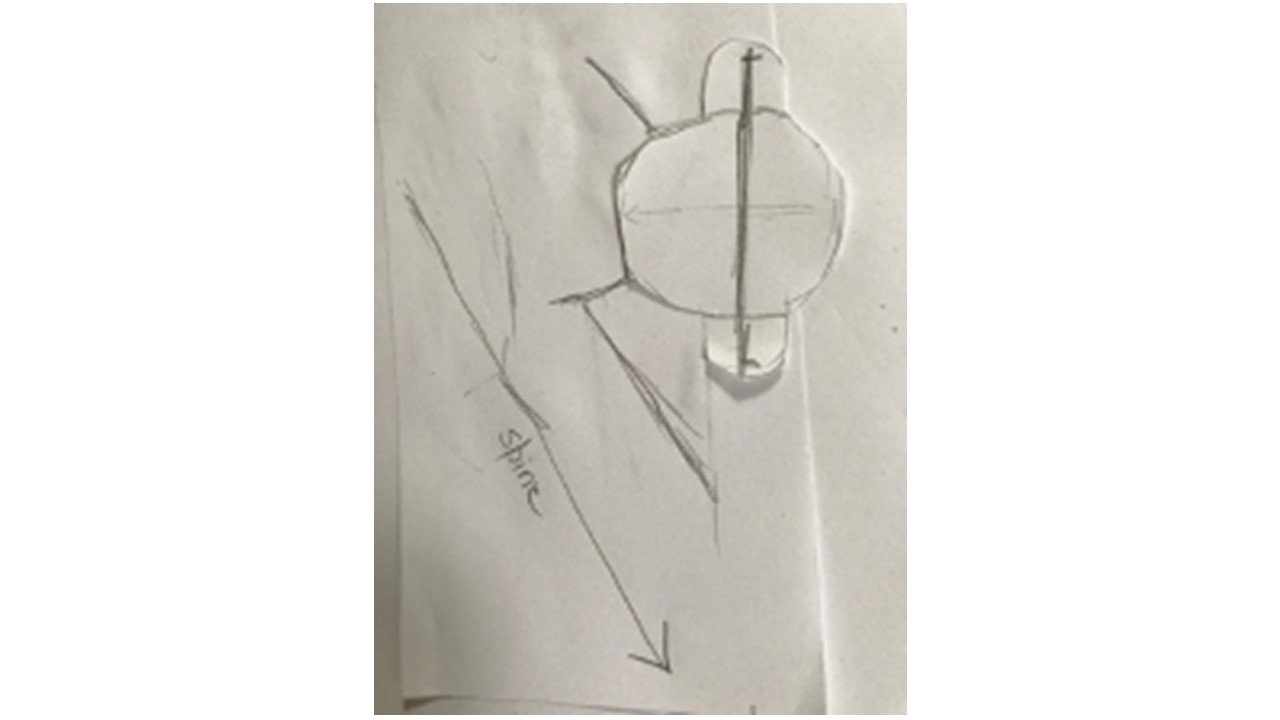
Can you see how Sally's breast falls relative to her tummy when she is at 45 degrees? Sally's breast-belly contour (which I'll refer to as breast-bellly contour S) is likely to allow her and her baby to fit together easily, without her needing to think much about it. This is because Sally has
-
Ample space between the under-surface of her breast and her abdomen for her baby to manouvre in
-
Excellent exposure of her breast's landing pad (ten centimeter diameter) for baby's face-breast bury
Because a baby needs good straight spinal alignment from his pelvis to the back of his head to be able to suck and swallow comfortably, he needs to come onto the breast like a little airplane, his shoulders (the wings) nice and straight on either side of his ear. We don't want his head and spine (the plane's body or fuselage) twisted or rotated off to the side, relative to the wings of his shoulders.
You can see the rotating effects of other breast-belly contours here and here. Once we know what's going on, it's not hard to make changes.
Sally's breast-belly contour means that her tummy won't interfere with the angle at which her baby's body and shoulders, and therefore her baby's face, come to the breast.
-
It will be easy for her to experiment with where she holds her baby vertically relative to her breast fall using micromovements
-
It will be easy for her to experiment with the angle of her baby's face-breast bury, without her tummy interfering with the angle at which her baby's face comes on to her breast, using micromovements.
Breast-belly contour is more about angles and the relationship between our breasts and belly, than about size and shape of our breasts or belly
Breast-belly contour is more about angles than about breast and tummy size and shape, although these factors do interact. We might say that Sally's breast is neither petite nor overly generous. But it is possible for women whose breasts are petite or generous to have a breast-bellly contour like Sally's.
It might seem that Sally has a flatter tummy, but in fact she might still have a delightfully round or ample tummy, and very generous breast - but her breasts are shaped so that they project a long way out above her tummy when her bra is down or off, with easy landing pad exposure and lots of room under her breasts for baby's body.
Of course, a woman with Sally's breast-belly contour can still have breastfeeding problems, because lots of other factors also affect fit and hold in breastfeeding (which you can find out about here).
The direction that Sally's nipple looks interacts with her breast-belly contour as she fits her baby into her body
You can find out about the different directions our nipples look and how this affects breastfeeding here.
As you can see in the sketch above, Sally's nipple looks directly out from her body. It doesn't look upwards and it doesn't look downwards. This is another reason why it's not hard for Sally to fit her baby into the contours of her body with a nice, deep, symmetrical face-breast bury. Although the distance between the tips of her baby's shoulders is wider than the baby's head, baby's shoulders have plenty of space so that the little head doesn't twist, and his face can bury in symmetrically to the nipple.
The sketches on this page are proportional (though they are otherwise very rough!) and use research-based average dimensions of a newborn's head from one side to the other, and the width between the baby's shoulder tips.
In the next three sketches, I'll show you breast-belly contours like Sally's, except with the nipple looking in three different directions.
-
The nipple looks out anywhere in a horizontal plane (either off to the side or in the midline)
-
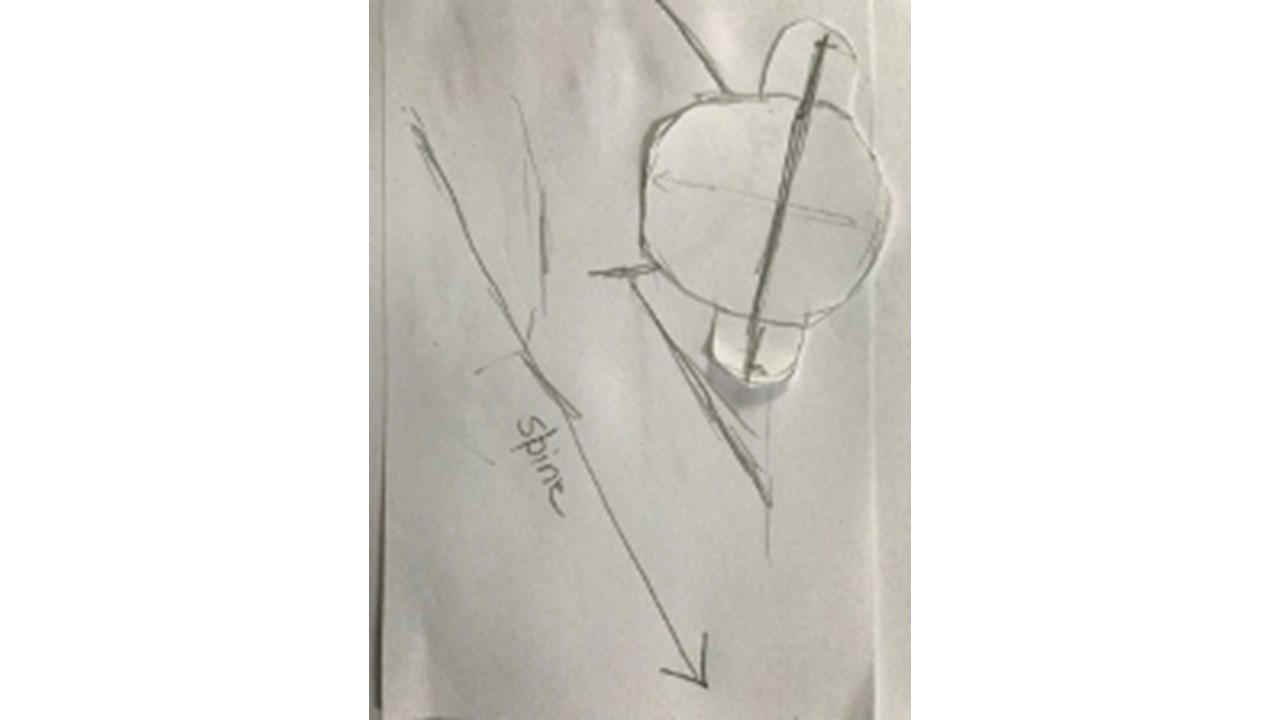
Somewhat downwards, anywhere in the horizontal plane (whether off to the side or in the midline), maybe by about 30 degrees from the horizontal plane
-
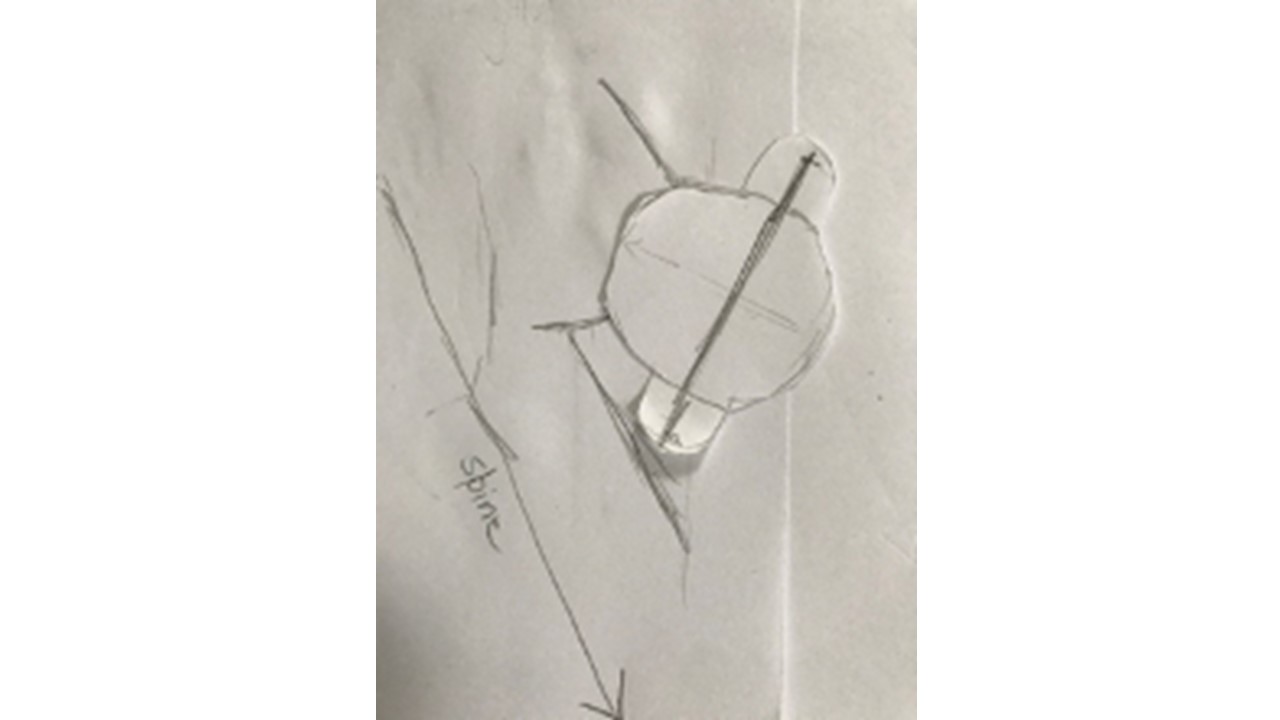
Even more downwards towards the ground (whether off to the side or in her midline), maybe by about 60 or 70 degrees from the horizontal plane.
Fitting baby into Sallly's breast-belly contour if her nipple looks somewhat downwards
It's not hard for Sally to fit her baby into the contours of her body with a nice, deep, symmetrical face-breast bury, even though her nipple is looking somewhat downwards in this case. Although the distance between the tips of her baby's shoulders is wider than the baby's head, baby's shoulders have plenty of space so that the little head doesn't twist, and his face can bury in symmetrically to the slightly downward-looking nipple.
Fitting baby into Sally's breast-belly contour if her nipple looks even more downwards
It's still not hard for Sally to fit her baby into the contours of her body with a nice, deep, symmetrical face-breast bury, even though her nipple is looking even more downwards. Although the distance between the tips of her baby's shoulders is wider than the baby's head, baby's shoulders have plenty of space so that the little head doesn't have to twist, and his face can bury in symmetrically to her rather downward-looking nipple.
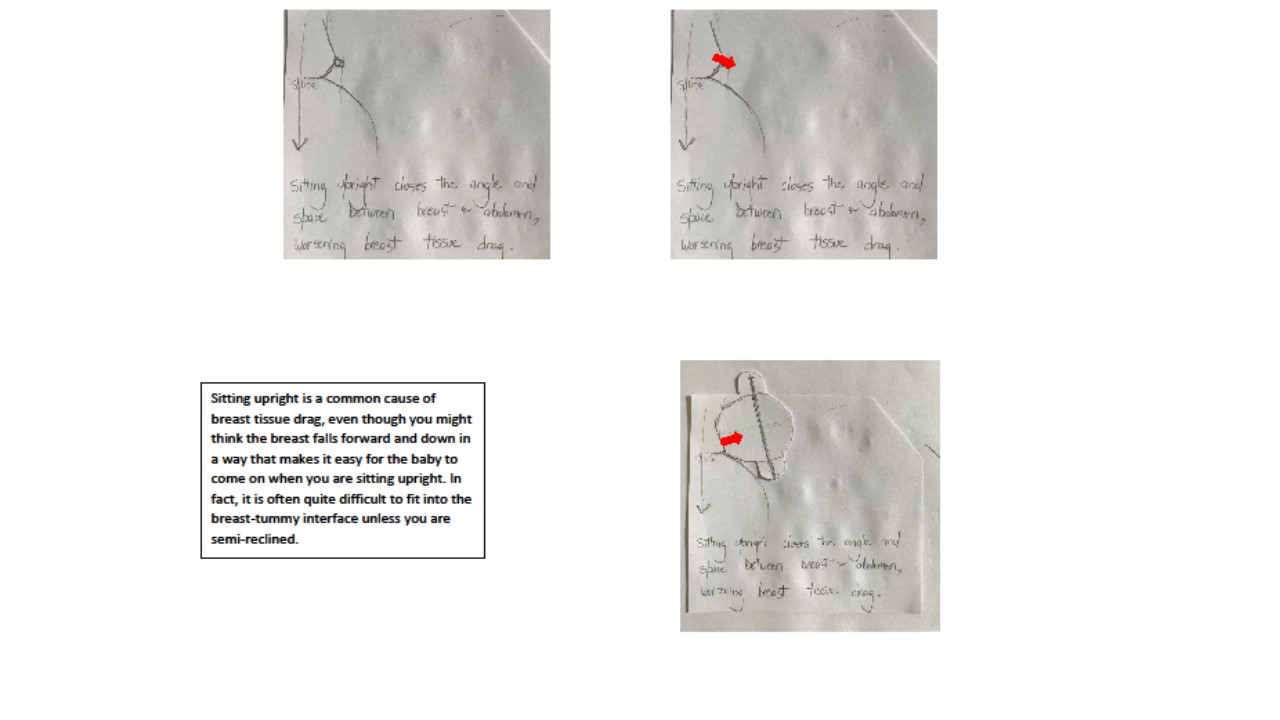
Sitting upright closes Sally's lap and might create nipple and breast tissue drag
You can see in the three small sketches below Sally's nipple looks slightly downwards when she's sitting upright, which is where the force of gravity falls through her nipple (red arrow in top left sketch). In the upright position, her breast-belly contour affects her baby's body and shoulders so that the vacuum that is created by the baby in her mouth as she suckles drags the nipple and breast tissue up in a direction that is different to where the nipple and breast tissue naturally rest with gravity (red arrow in bottom left sketch). This can cause nipple pain or a baby who fusses and backarches a lot at the breast.
-
You can find out about the directions nipples look and how this affects fit and hold in breastfeeding here.
-
You can find out about breastfeeding with petite breasts here, and with generous breasts here.
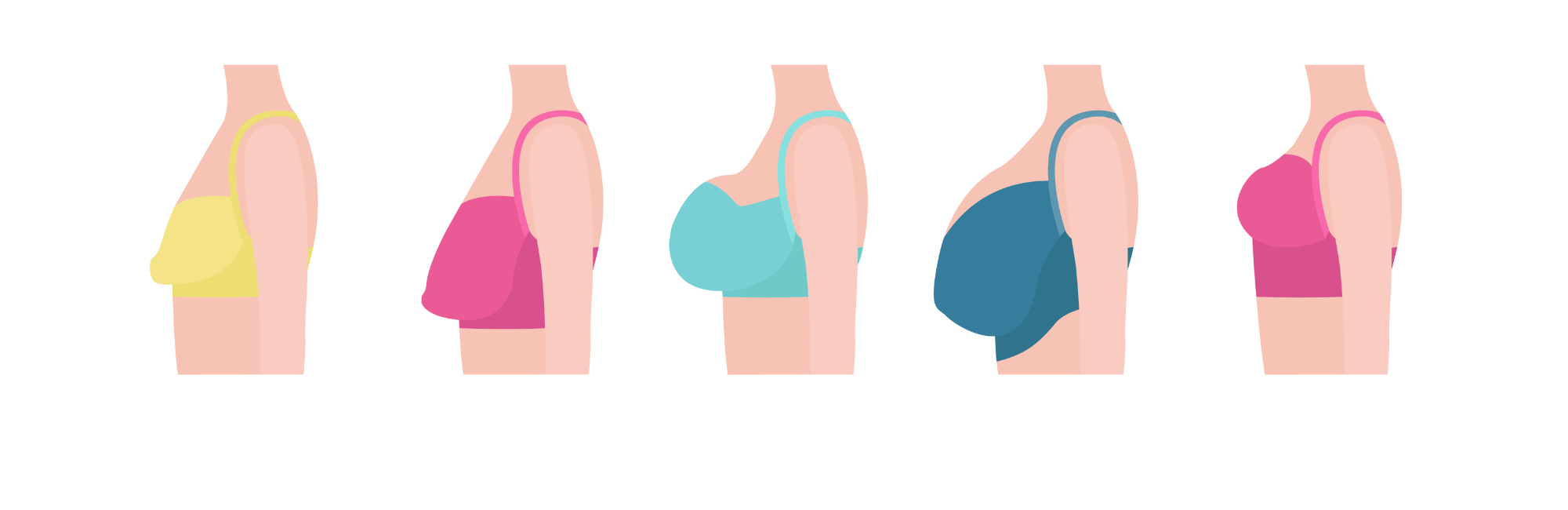
Getting clever about noticing breast-belly contour
Now when we look at the ladies in the coloured drawings below, we can muse together on whether or not they would have a breast-belly contour like Sally's if they removed or opened up their bra in a semi-reclined position for breastfeeding, or whether they have a different kind of breast-belly contour. It can be hard to guess, though, because a bra changes the breast-belly contour, as does sitting upright or standing up!
Here's what I think! I'm guessing that the ladies in the light green and teal bras are likely to have a breast-belly contour like Sally's. What do you think?
You can find out about the breast-belly contours which are often (though not always!) found with
If the mother and baby in the photo at the very bottom of this page on the stripey blue sheets had any breastfeeding problems, I would suggest she brings her little one in deeper to her breast, for a better face-breast bury since we can still see the little one's lips. When she draws her baby in deeper, she may need to use micromovements to get rid of any breast tissue drag that bringing him in deeper creaetes. You can find out about the gestalt method in side-lying here.

Recommended resources
PBL Foundations
What's useful to notice in the mirror before you bring baby on to your breast?
What does the gestalt method mean by the 'landing pad'?
PBL Intermediate
Working breasts are diverse on the outside
What's helpful to know about fitting baby into your petite breast?
Woman-centred language and weight-inclusive care of breastfeeding and lactating women
Selected references
Douglas PS, Geddes DB. Practice-based interpretation of ultrasound studies leads the way to less pharmaceutical and surgical intervention for breastfeeding babies and more effective clinical support. Midwifery. 2018;58:145–155.
Douglas PS, Perrella SL, Geddes DT. A brief gestalt intervention changes ultrasound measures of tongue movement during breastfeeding: case series. BMC Pregnancy and Childbirth. 2022;22(1):94. DOI: 10.1186/s12884-12021-04363-12887.
Douglas PS, Keogh R. Gestalt breastfeeding: helping mothers and infants optimise positional stability and intra-oral breast tissue volume for effective, pain-free milk transfer. Journal of Human Lactation. 2017;33(3):509–518.
Verspyck E, Goffinet F, Hellot MF, Milliez J, Marpeua L. Newborn shoulder width: a prospectie study of 2222 consecutive measurements. British Journal of Obstetrics and Gynaecology. 1999;106:589-595.
Ismail A-QT, Fritze A, Rudiger M, Ismail K. Obstetric forceps dimensions and the newborn head biometry: time for an update. European Journal of Obsetrics and Gynecology and Reproductive Biology. 2021;25;6:270-273.