
Janine and two other generous-breasted women demonstrate fit and hold strategies which they found helpful
What helps if you have a generous breast and face fit and hold challenges?
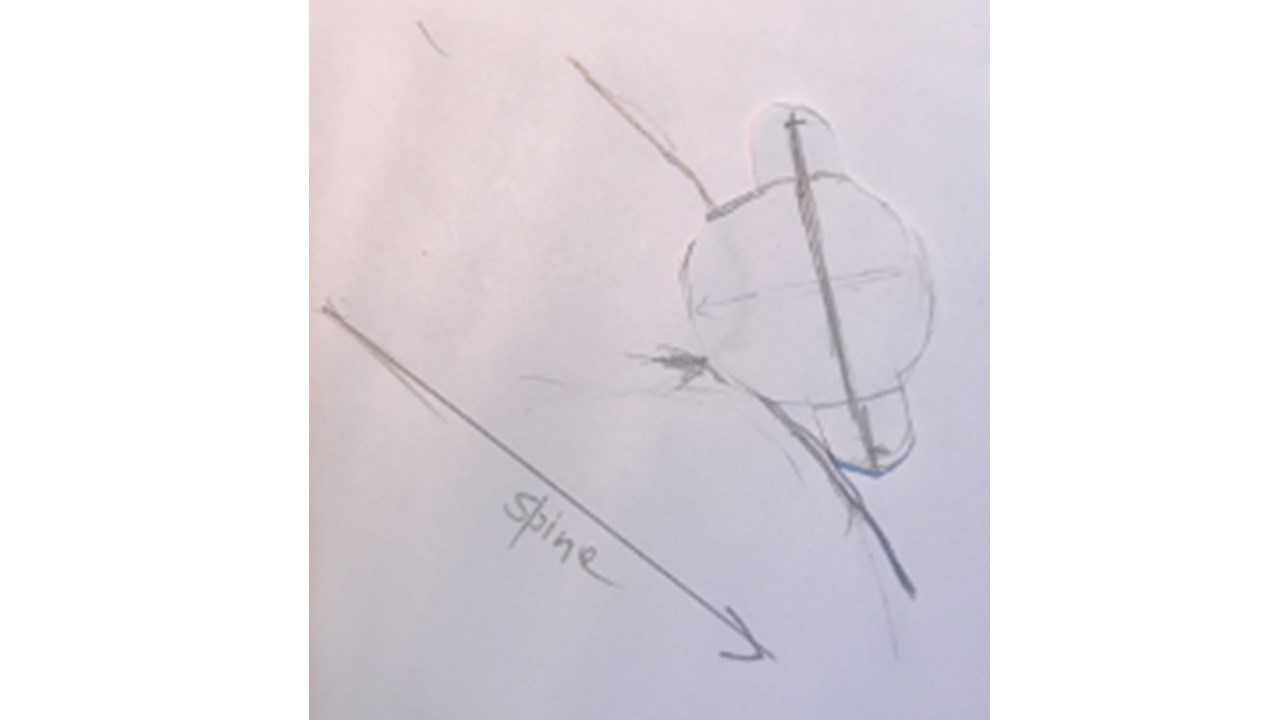
Do you have a wonderfully generous breast? Do you have a generous breast with downward looking nipples? Here is a drawing of Janine's breast-belly contour when she is reclined at 45 degrees. Perhaps your own precious body and breasts are similarly shaped?

Janine was having a lot of difficulty bringing her baby on to the breast. Once baby did come in, she either pulled off or seemed to slip off very quickly.
You can see that Janine has little or no space between the under surface of her breast and her abdomen to fit the baby in, and she is unable to expose a 10 cm diameter landing pad in a 45 degrees semi-reclined position. Unless she puts in place some other strategies, breast tissue drag is inevitable, causing difficulty bringing the baby on, nipple pain, fussing at the breast, and pulling off the breast.
This is because when little shoulders that need to twist away over the curve of our tummies, it is hard for that little one's face to bury into the breast without causing nipple and breast tissue drag. You can see the problem in the sketch that includes her baby, below.
There are some mother-baby pairs for whom a breast-belly contour like Janine's isn't a problem, and everything works out just fine without help. But for many women and their babies with breast-belly contour like Janine's there is either nipple pain, or lots of fussing and distress for the baby because he has difficulty coming onto, or staying on, the breast.
Often baby's difficulty coming on to the breast in this situation is blamed on a less prominent nipple. But it's the biomechanics that matter, before all else, and not so much our nipple's size and shape!
How Janine works through her and her baby's fit and hold challenges
.jpeg)
Here are the steps we took together, which resolved the problems.
-
We rolled up Janine's bra, by rolling the cup tightly inwards. Even with her bra rolled up tightly under her breast, you can see in the photo immediately above why Janine's baby was having difficulty coming on to her breast, with lots of fussing. Another woman in the same situation might be experiencing nipple pain and damage.
-
We used a rolled up facecloth under Janine's breast, in addition to her rolled up bra. You can find a demonstration of how to create the right cloth roll here. The roll needs to be tucked up very high under Janine's breast, where it meets her rib-cage, to better expose the landing pad. I discuss how you might experiment with a facecloth roll the way Janine and I did in greater detail here.
-
Sometimes, it works best to have two facecloths need to be laid against each other, then folded in half, then tightly rolled up work best. I describe different ways of making a cloth roll work here.
-
Sometimes the roll is best not placed right at the junction of the woman's breast and her ribcage, because her breast just falls right over the roll and the landing pad isn't well exposed. In her case, bringing the roll somewhat forward under breast as long as it doesn't get in the way of baby or the landing pad can work best.
-
.jpeg)
-
Janine reclined back at about 45 degrees, with a soft pillow in the small of her back. This opened up her lap and also helped expose the landing pad of her breast
-
Sometimes being very reclined, even more than 45 degrees if you can do it, better helps open up your lap and breasts so that the baby comes up under your breasts, especially while you and baby are still working things out together.
-
You may not be able to see much, but that's normal for many women. You just do it all by feel, experimenting. Your baby has the inbuilt reflexes to get on, if you keep experimenting and applying the gestalt method. Leaning forward so that you can see can actually worsen breastfeeding problems.
-
-
Some woman use their hand to lift their breast just a little, and also to shape some breast tissue including the nipple between their fingers to form a 'teat' when they bring baby on. If you are experimenting with this, try not to move your breast far from where our breast naturally wants to fall, and use the baby's face to support the breast once you bring the baby on, so that there is no drag of the tissue out of his or her mouth. Change back to having your forearm under the baby's head for micromovements just as soon as possible. Some women with contour J find this works best for them, as long as they are aware of the risk of creating more breast tissue drag.
-
Some women use their upper arm to hold the breast forward, or wear a bra with a supportive side strap, so that their generous breast doesn't fall too far off to the side. The photo of baby 1, immediately below, shows a mother using her upper arm to support her breast so that the nipple looks more forward, rather than the breast and nipple falling off to her side.
-
To begin with, you might use your opposite hand to tuck the breast forward and then bring your upper arm in to support it in that position.
-
This does immediately limit what you can do with your forearm, which is your lever for creating micromovements and getting rid of breast tissue drag, but women experiment with these ideas and compromise and find something that works.
-
Here's a photo of a generous-breasted woman using her upper arm to stabilise her breast so that her breast and nipple look more foreward.

-
We tucked Janine's little one up as high as possible underneath the opposite breast (which the gestalt method calls a ribcage wrap), so that her breast rests on the baby's hip and body, giving baby the best biomechanics for breastfeeding. I'm always saying to women that I know this might seem weird, but it typically transforms breastfeeding for newborns with problems. As the baby grows longer, the ribcage wrap doesn't work as well because baby kicks off the back of the chair, and baby is slightly diagonal across the mother's body.
-
We made sure baby's lower arm was wrapped around Janine's side, not tucked up close to her body, which makes it harder for baby to come up under the breast. Sometimes the baby needs to be positioned so that she is looking on a slant up towards the ceiling, to come on just where the nipple wants to look without creating nipple and breast tissue drag.
-
We used micromovements to ensure the little one had a symmetrical, deep face-breast bury, and was relaxed and stable during breastfeeding.
-
Janine couldn't really see much of what her baby was doing as she brought the baby on. That's a normal occurence. But your baby has inbuilt reflexes to come onto the breast, so you're just doing it by feel, continuing to experiment.
Case 1. What might better help this newborn come onto and stay on her mother's generous breast?

In this photo, above, the woman is more reclined than you can detect. She is using her upper arm, forearm, and importantly, the baby's face, to support her breast. The baby is feeding well in this position, although the spine is not as aligned as I like to see - there is a twist to the head, as if the baby might be falling away from the breast. Lying back even further could help.
The most important change this mother could if the baby was continuing to fuss or she continued to have nipple pain is to lift the breast on the right, and bring the baby's bottom up under her breast, so that there is a true, tight rib-cage wrap with the breast resting on top of the baby. Also, it might help to bring her forearm slightly out towards the viewer, so that baby's head is better supported, and the mother has more control over helping the baby bury his face into her breast.
It may be, though, that this lady's been experimenting with gestalt method and has found that this compromise, of offering some support to her breast with her forearm even though it affects what she can do with the baby's head, is most workable for her and her baby.
She then uses the baby's face to stabilise her generous breast. The baby's deep face-breast bury, helped by a very semi-reclined position, means that there is no breast tissue drag.

Case 2. What might better help this newborn come onto and stay on her mother's generous breast?


This woman's nipple pain in the two photos above immediately resolved with the gestalt method. She had previously been told to lift her breast, shape it, and press the breast towards the baby's mouth, which resulted in drag of breast tissue in her mouth and pinching of the nipple as the feed progressed. I have also placed a tightly rolled up face-washer under the breast she is feeding from.
In the first photo, she isn't applying a paddle hand between the shoulder blade and her wrist is at risk of pain because it is tightly flexed in, to rest against her baby's back. It's not that anything is wrong, but there are reasons why the paddle hand optimises fit and hold, found here, and it's important to protect women's wrists from repetitive strain injury, which is not uncommon when caring for a baby.
This sculpture below was carved from limestone 30,000 years ago, and is known as the Woman from Willendorf. She stands about 11 centimetres tall. Scholars believe she is an ancient celebration of the divine powers of female fertility, power, and beauty. She has such wonderfully generous breasts! If you want to, you could click here into Wickipedia to see a side-view of the glorious breast-belly contour of this generous-bodied, generous-breasted Woman from Willendorf.
{kind=link}

Acknowledgements
I gratefully acknowledge the generosity of the women who agreed to share their experiences with their babies in these photos, for the sake of helping others.
Recommended resources
PBL Intermediate
How Janine uses a rolled up facecloth to better expose her generous breast's 'landing pad'
Why it's often best not to shape your breast with your hand though some women need to
Woman-centred language and weight-inclusive care of breastfeeding and lactating women